What Physician-Led Testosterone Evaluation Actually Looks Like
By Dr. Kyle Kingsley, MD
Last reviewed by a licensed physician — 2026-03-23
Many men in Edina and Minneapolis reach a point where something feels off — energy levels have dropped, sleep is poor, motivation has stalled, and libido has quietly disappeared — but they can’t pinpoint why. Testosterone replacement therapy (TRT) is a meaningful option for men with clinically confirmed low testosterone, but determining candidacy requires more than a single blood draw. It requires correlating symptoms with laboratory values, ruling out other causes, and making a well-informed clinical decision with a physician who understands the full picture.
In clinical practice, the path to TRT candidacy is often misunderstood. Some men assume low energy and reduced drive are simply signs of aging, and they delay evaluation for years. Others receive a “normal” testosterone result from a basic panel and are told nothing is wrong — even though their free testosterone or SHBG levels tell a different story. Physician-led evaluation is designed to cut through that confusion and provide answers grounded in evidence.
What ‘Low T’ Actually Means Clinically
Low testosterone — medically termed hypogonadism — is defined by the body’s inability to produce testosterone at levels sufficient to maintain normal physiological function. According to the American Urological Association’s Testosterone Deficiency Guideline, testosterone deficiency is confirmed when total testosterone falls below 300 ng/dL on two separate morning measurements, accompanied by symptoms consistent with low androgen levels.
There are two distinct categories. Primary hypogonadism originates in the testes themselves and typically results in elevated LH and FSH as the pituitary signals the testes to produce more. Secondary hypogonadism originates in the hypothalamic-pituitary axis — this pattern is more common in men with obesity, sleep apnea, or chronic stress. Understanding which type is present matters clinically, because the underlying cause influences whether TRT is the right intervention or whether addressing a root cause first is more appropriate. It is also essential to distinguish clinically low testosterone from the natural 1–2% annual decline in levels that occurs with aging — not every drop below a reference range is hypogonadism.
Recognizing the Symptoms That Actually Point to Low Testosterone
The symptom profile of low testosterone is broad, and no single symptom is diagnostic. The most commonly reported include persistent fatigue that does not improve with adequate sleep, reduced or absent libido, difficulty achieving or maintaining erections, loss of lean muscle mass despite regular training, and increased visceral body fat. Men also frequently report cognitive changes such as difficulty concentrating and mental fog. Mood-related symptoms — depression, irritability, reduced motivation, and emotional flatness — are equally significant and often overlooked entirely.
None of these symptoms is specific to testosterone deficiency. Fatigue may reflect sleep apnea, thyroid dysfunction, or depression. Low libido can stem from relationship stress or medications. The purpose of clinical evaluation is to determine, through structured history-taking and laboratory analysis, whether low testosterone is a contributing factor — and whether treating it is clinically appropriate. Men who have been experiencing these symptoms for months or years often find that a proper evaluation finally gives them an explanation and a clear path forward.
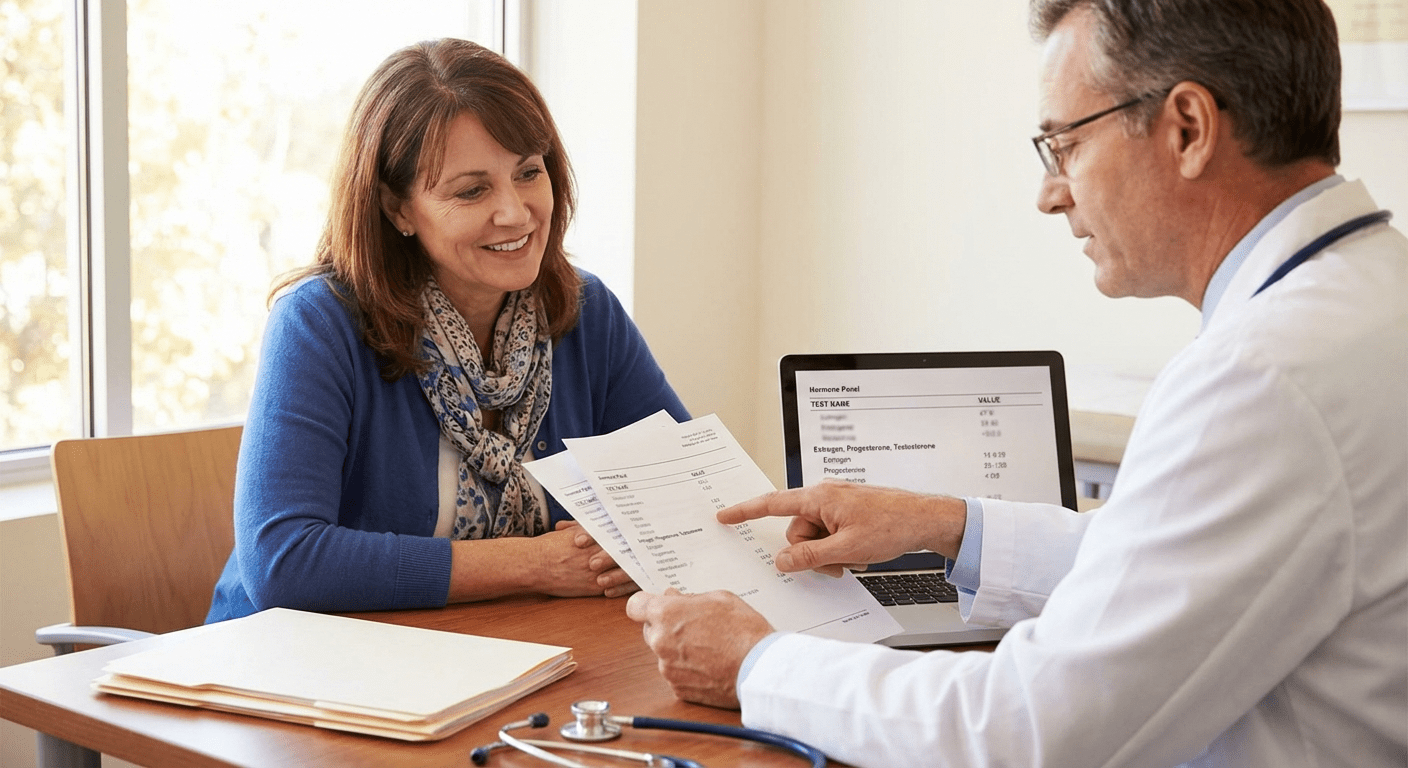
What Testosterone Testing Actually Involves
Testosterone is best measured in the morning, typically between 7:00 and 10:00 AM, when levels peak due to circadian rhythm. An afternoon blood draw may understate true levels and lead to false reassurance. A comprehensive testosterone panel includes total testosterone, free testosterone, sex hormone-binding globulin (SHBG), luteinizing hormone (LH), follicle-stimulating hormone (FSH), and estradiol. A complete metabolic panel and CBC round out the baseline picture by identifying conditions that could affect hormone metabolism or influence treatment risk.
Confirming hypogonadism requires two separate blood tests on different days, because testosterone levels can fluctuate meaningfully between draws. Free testosterone below 65 pg/mL can indicate deficiency even when total testosterone appears borderline, particularly in men with elevated SHBG. These nuances are exactly why having a physician interpret results — rather than relying on an automated range flag — is critical to accurate diagnosis.
How Lite Medical Evaluates TRT Candidates in Edina
At our Edina clinic, the TRT evaluation process is physician-led from the first appointment. We begin with a structured intake covering symptom history, onset, severity, and functional impact. We review medications, sleep patterns, and any comorbid conditions that could influence hormone levels or treatment safety. Conditions that would disqualify a man from TRT — including untreated polycythemia, active prostate cancer, uncontrolled sleep apnea, or a desire to preserve fertility — are identified before any treatment decision is made.
Laboratory results are reviewed in context, not in isolation. A total testosterone of 285 ng/dL in a 45-year-old man with significant fatigue, low libido, and muscle loss tells a different clinical story than the same value in a man who feels entirely well. Our evaluation correlates both dimensions before a recommendation is made. We also discuss realistic expectations — what TRT can and cannot address, what the monitoring schedule looks like, and what the cash-pay cost structure involves. If you’re ready to understand your baseline, scheduling a discovery intake is the first step.
Understanding the Benefits and Risks of TRT
When prescribed appropriately and monitored properly, TRT offers meaningful evidence-supported benefits for men with confirmed hypogonadism. Improvements in energy, libido, erectile function, mood, and body composition — including increased lean muscle and reduced body fat — are among the most consistently reported outcomes. Bone mineral density also improves with sustained therapy, which has long-term relevance for men at risk for osteoporosis.
However, TRT is not without risk. Erythrocytosis — an elevation of red blood cell count — is the most clinically significant risk and requires periodic hematocrit monitoring to prevent clotting complications. TRT suppresses the hypothalamic-pituitary-gonadal axis, reducing sperm production and causing testicular atrophy; men who wish to remain fertile should discuss alternatives before starting. Prostate health requires baseline PSA measurement and periodic re-evaluation. The Endocrine Society’s Clinical Practice Guidelines for Testosterone Therapy provide a comprehensive risk-stratification framework, and we adhere to those standards in our clinical decision-making. Sleep apnea can worsen on TRT, so men with a history of apneic episodes warrant evaluation before treatment begins.
TRT Care Across the Twin Cities — Including Rochester
Lite Medical serves men throughout the Minneapolis–Saint Paul metro and greater Minnesota. Our Edina clinic is the primary option for men in the southwest metro and Minneapolis, while men in southeast Minnesota can receive the same physician-led evaluation and TRT management at our Rochester clinic. Every Lite Medical location operates on the same cash-pay, physician-led model — no insurance paperwork, no referral chains, and no waiting months for a specialist appointment. Cash-pay care also means the physician recommends testing that is clinically appropriate, not just what an insurer will authorize.
Taking the Next Step Toward Testing
If you’ve been experiencing fatigue, low libido, mood changes, or reduced physical performance and you suspect testosterone may be a factor, the most important step is a proper physician evaluation — not guessing, not relying on over-the-counter supplements as a substitute for diagnosis, and not obtaining testosterone from unmonitored sources. TRT affects multiple organ systems simultaneously and requires individual calibration over time. At Lite Medical, we will not prescribe TRT to a man who doesn’t need it, and we will not withhold it from a man who does. Learn more about our physicians and clinical philosophy at litemedicalclinic.com/about, and take the first step toward a clear answer about your testosterone health.
Frequently Asked Questions
How do I know if I’m actually a candidate for TRT in Edina?
You may be a TRT candidate in Edina if you have both clinical symptoms — such as fatigue, low libido, loss of muscle, or mood changes — and laboratory confirmation of testosterone deficiency, defined as total testosterone below 300 ng/dL on two separate morning blood draws. The evaluation at Lite Medical’s Edina clinic correlates your symptom severity with lab results and rules out other causes before any treatment recommendation is made. A man with symptoms but borderline labs, or labs without symptoms, would typically require further workup before being considered an immediate candidate.
What testosterone level is too low for men in Minneapolis?
According to the American Urological Association, a total testosterone level consistently below 300 ng/dL combined with symptoms of hypogonadism is the general threshold for considering testosterone replacement therapy. Some men with levels in the 300–400 ng/dL range may also experience symptoms if free testosterone is low due to elevated SHBG — which is why a comprehensive panel matters beyond just the total number. There is no single cutoff that applies universally; the full clinical picture always guides the final interpretation.
What are the risks of TRT, and how are they managed at Lite Medical?
The primary risks of TRT include erythrocytosis (elevated red blood cell count, which increases clotting risk), suppression of natural sperm production, testicular atrophy, and potential worsening of sleep apnea. At Lite Medical, we manage these risks through scheduled monitoring: hematocrit is checked every 3–6 months, PSA is assessed at baseline and annually, and a full symptom review occurs at each visit. Men who wish to preserve fertility are counseled about alternatives before starting TRT, since therapy can significantly reduce sperm production.
How often is testosterone monitored once therapy begins?
Once TRT is initiated, testosterone levels are typically measured at the 6–8 week mark to assess response and guide dose adjustment, then every 3–6 months once a stable therapeutic level is achieved. Hematocrit, PSA, and a metabolic panel are included in the monitoring schedule. At Lite Medical’s Edina clinic, monitoring visits also include a symptom review — lab values alone do not capture the full clinical picture, and dosing adjustments are made based on both trends and how the patient is actually functioning.
What does TRT cost at Lite Medical’s Edina clinic?
As a cash-pay clinic, Lite Medical does not bill insurance for TRT services, and pricing is transparent and discussed at the time of your discovery intake. The initial consultation and comprehensive testosterone panel, physician visits, and monitoring labs are priced individually without surprise fees. Many men find that cash-pay care at Lite Medical is cost-competitive with the copays and deductibles associated with navigating insurance-based hormone care — and they receive significantly more physician time and individualized attention. Contact the Edina clinic directly for current pricing on the initial evaluation and ongoing management.
Is physician-led TRT available to men across the Minneapolis area?
Yes — Lite Medical’s Edina clinic, located at 4388 France Ave S Suite 210, Edina, MN 55410, serves men throughout Minneapolis, Edina, Eden Prairie, Bloomington, and the southwest metro. Men in southeast Minnesota can be seen at our Rochester clinic for the same physician-led testosterone evaluation and management. All Lite Medical TRT programs are supervised directly by a physician, include comprehensive baseline and monitoring labs, and operate on a cash-pay model that allows for fully personalized care without insurance restrictions.

References
- American Urological Association — Testosterone Deficiency Guideline — Establishes the clinical definition, diagnostic thresholds (below 300 ng/dL), and evidence-based management recommendations for male hypogonadism.
- Endocrine Society — Clinical Practice Guidelines for Testosterone Therapy in Men — Provides a comprehensive framework for patient selection, risk stratification, and monitoring protocols for testosterone replacement therapy.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The information provided is not intended to diagnose, treat, cure, or prevent any medical condition. Individual results from testosterone replacement therapy vary and are not guaranteed. TRT should only be initiated after a thorough evaluation by a qualified, licensed physician. Please consult a healthcare provider for personalized medical guidance.